Slipped Vertebra (Spondylolisthesis): Symptoms and Treatments
Dr Colum Nolan
Senior Consultant Spine & Neurosurgeon
MB, BCh, BAO, LRCPSI, MRCSI, FRCSI (Neurosurgery)
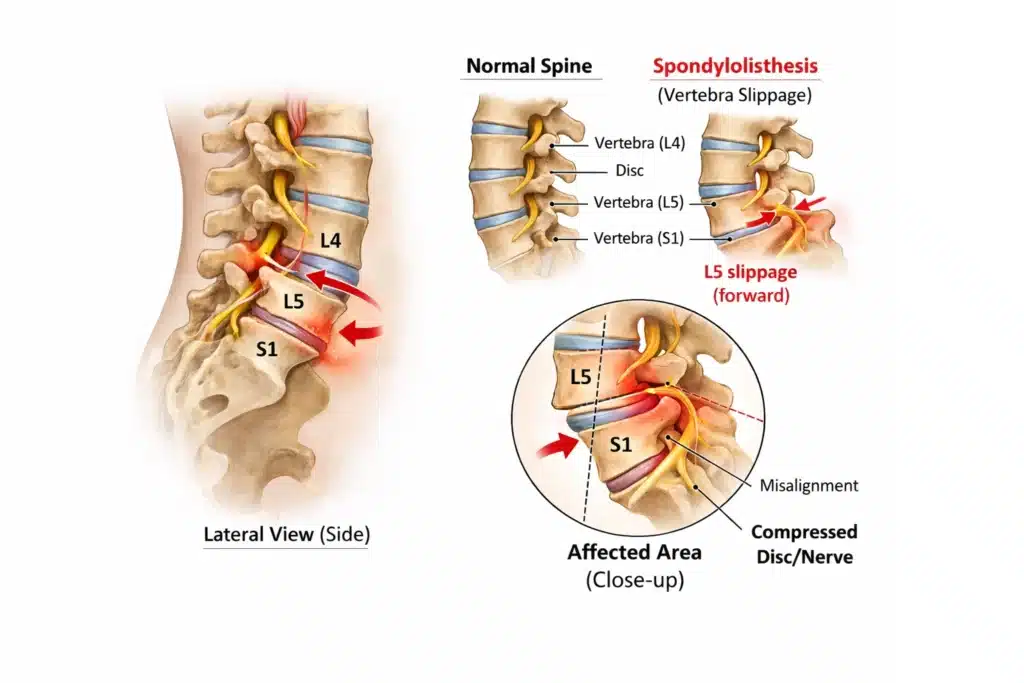
A “slipped vertebra” usually refers to spondylolisthesis, where one vertebra slips forward over the one below it. This shift can narrow the space where spinal nerves exit, leading to nerve irritation or compression and pain that may travel into the buttock or leg.
How Spondylolisthesis Affects the Lower Back
Spondylolisthesis most commonly occurs in the lumbar spine (lower back). Some people have a slip found on X-ray but feel fine. Others develop symptoms because the slip:
Strains the joints and soft tissues in the back, and/or
Reduces space for nerves, causing leg symptoms.
The impact depends on factors such as the degree of slip, whether there is instability, and whether the slip contributes to spinal canal or foraminal narrowing.
Treatment is typically stepwise, guided by your symptoms, function, and whether nerves are involved.
Many people improve with conservative care, which may include:
Activity modification (avoiding painful positions and repeated heavy loading during flare-ups)
Medication for pain or inflammation, when appropriate
Heat or cold therapy for symptom relief
Physiotherapy to improve core strength, hip flexibility, and movement control (The aim is to support spinal stability and reduce irritation.)
If nerve-related pain is a key feature, additional options may be considered.
When imaging and symptoms suggest nerve irritation, targeted injections (such as an epidural or nerve root injection) may be used to reduce inflammation and improve pain temporarily, supporting rehabilitation.
Surgery is usually considered when:
Symptoms remain significant despite a structured course of non-surgical treatment
Pain continues to limit daily activities or walking tolerance
There is significant or progressive weakness, or clear nerve compression on imaging
The goals of surgery are to relieve pressure on nerves (decompression) and, when needed,stabilise the spine (fusion).
Frequently Asked Questions about Spondylolisthesis
What is the difference between a slipped vertebra and a slipped disc?
Many cases are managed effectively with conservative treatment, especially when symptoms are mild to moderate, and there is no progressive weakness.
Does the “grade” of slip determine how serious it is?
Not always. The degree of slip matters, but treatment decisions usually depend more on symptoms, function, and nerve findings.
Should I get an MRI?
MRI is most useful when there are leg symptoms suggesting nerve involvement, or when symptoms persist despite initial care.
Medical disclaimer
This page is for general education and does not replace a medical consultation. If you have severe symptoms, worsening weakness, or bladder/bowel changes, seek urgent medical attention.
Our Spine & Neurosurgeon in Singapore
Dr Colum Nolan
MB, BCh, BAO, LRCPSI, MRCSI, FRCSI (Neurosurgery)
Dr Colum Nolan is a Senior Consultant Neurosurgeon with over 20 years of experience, specialising in minimally invasive spine (keyhole) surgery and other spine procedures.
A graduate of the Royal College of Surgeons in Ireland, Dr Nolan underwent neurosurgical training in Ireland and Australia, followed by a fellowship in complex spine surgery at Addenbrooke’s Hospital, Cambridge, as well as rotations at the Orthopaedic Spine Unit in Norfolk and Norwich Hospital.
Dr Colum is committed to delivering compassionate, patient-centred care, combining surgical precision with a genuine dedication to improving his patients’ quality of life.
Get in touch
Make an Enquiry or Request an Appointment
Our friendly team is here to serve you. For urgent enquiries and appointment requests, please call or WhatsApp us directly.